The hypothalamic-pituitary-adrenal (HPA) axis
The normal production of cortisol is controlled by the HPA axis, a negative feedback loop that adapts to multiple factors2,5
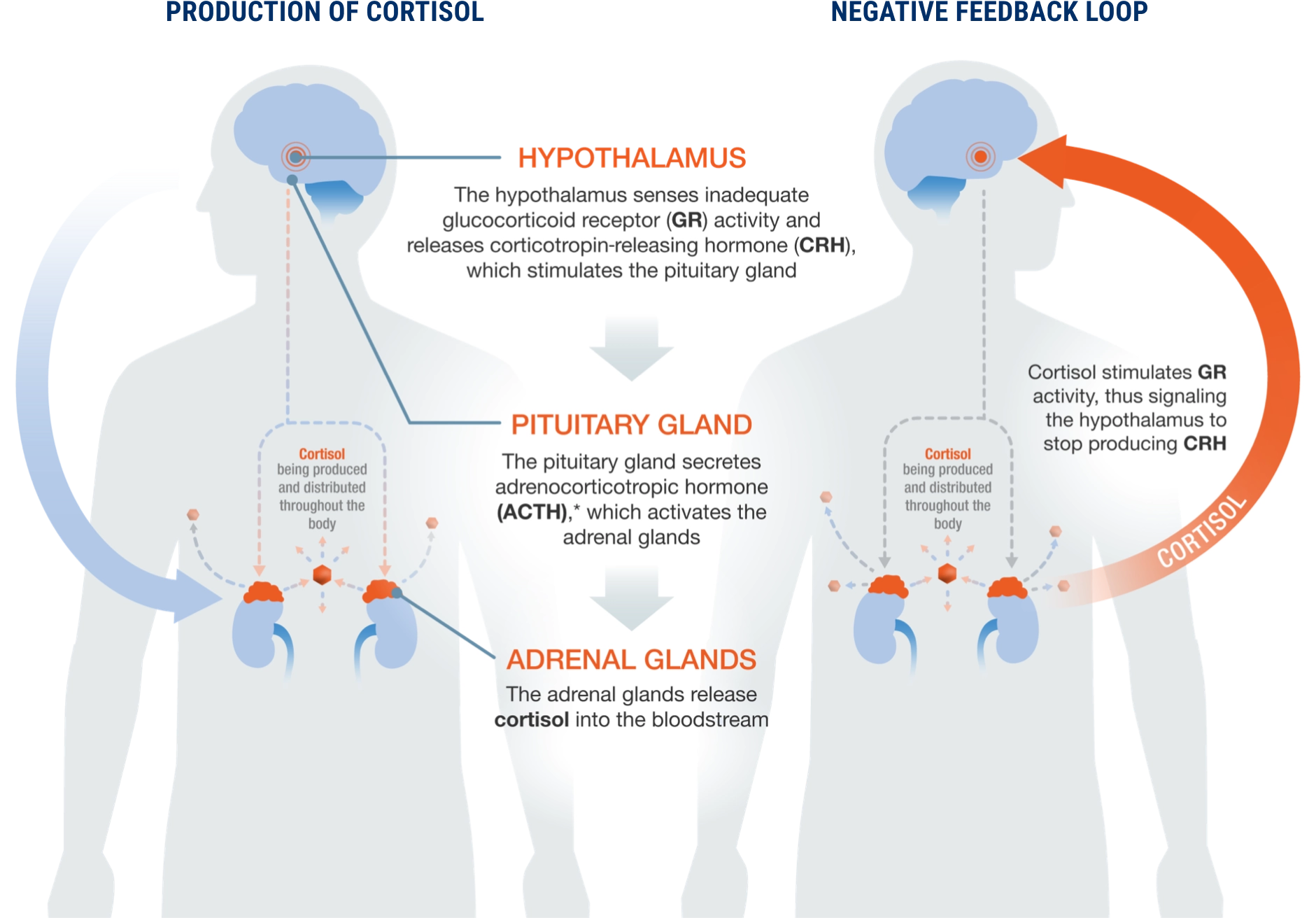

Cortisol is the most abundant endogenous glucocorticoid in the human body. It plays an important function in regulating physiological processes, including1,2:
Left untreated, over time, excess cortisol can negatively affect the body and cause multisystemic dysfunction, including increased risk for cardiovascular disease.3,4
The normal production of cortisol is controlled by the HPA axis, a negative feedback loop that adapts to multiple factors2,5
*ACTH also stimulates the release of DHEAS into the bloodstream. Low-serum DHEAS levels have been shown to be a marker of excess cortisol in patients with ACTH-independent hypercortisolism.6
Hypercortisolism occurs when the body is exposed to high levels of cortisol. There are 2 general causes of endogenous hypercortisolism.5
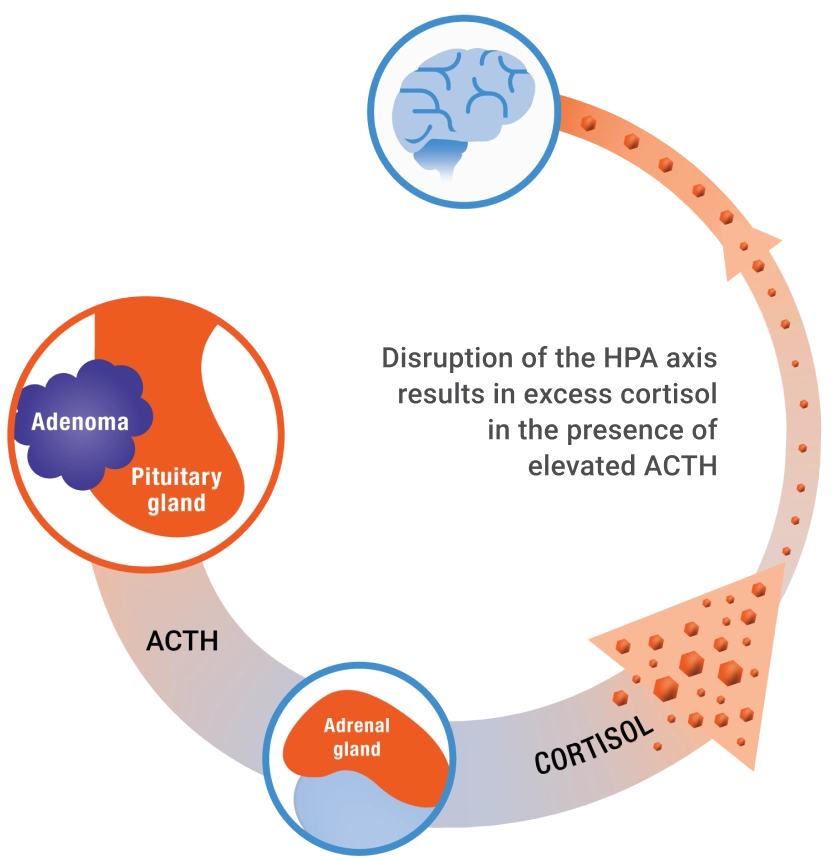
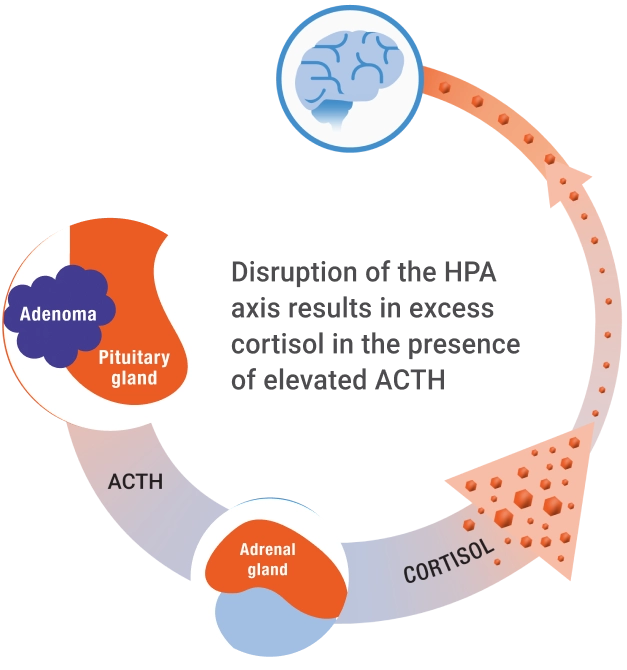
Secretion of ACTH from a pituitary adenoma stimulates the adrenal glands to secrete excess cortisol (Cushing disease).
Secretion of ACTH from an ectopic tumor stimulates the adrenal glands to secrete excess cortisol.

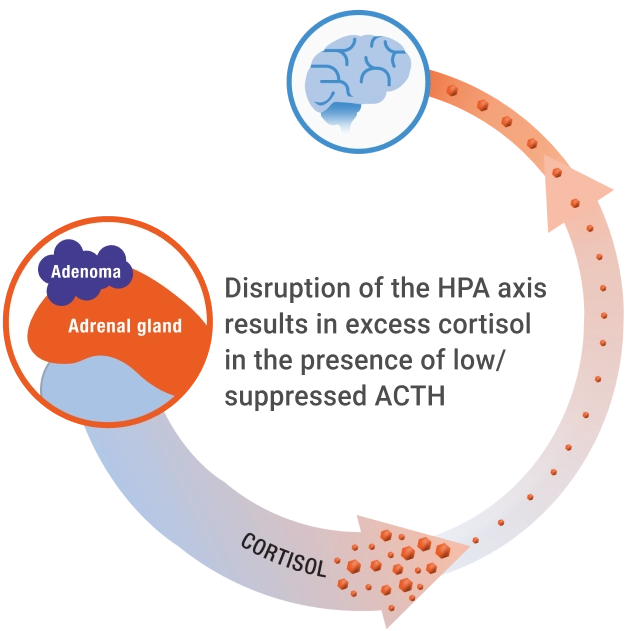
Secretion of cortisol from an adrenal adenoma causes excess autonomous cortisol secretion (Cushing syndrome).
Learn more about the types of hypercortisolism
Nearly 1 in 4 patients with difficult-to-control T2D had endogenous hypercortisolism7
The 1-mg dexamethasone suppression test detects all etiologies of hypercortisolism8
References
1. Jovanovic F, Jovanovic V, Knezevic NN. Cells. 2023;12(8):1178. doi:10.3390/cells12081178 2. Dickerson SS, Kemeny ME. Psychol Bull. 2004;130(3):355-391. doi:10.1037/0033-2909.130.3.355 3. Raff H, Sharma ST, Nieman LK. Compr Physiol. 2014;4(2):739-769. doi:10.1002/cphy.c130035 4. Di Dalmazi G, Vicennati V, Garelli S, et al. Lancet Diabetes Endocrinol. 2014;2(5):396-405. doi:10.1016/S2213-8587(13)70211-0 5. Guaraldi F, Salvatori R. J Am Board Fam Med. 2012;25(2):199-208. doi:10.3122/jabfm.2012.02.110227 6. Chiodini I, Ramos-Rivera A, Marcus AO, Yau H. J Endocr Soc. 2019;3(5):1097-1109. doi:10.1210/js.2018-00382 7. Buse JB, Kahn SE, Aroda VR, et al. Diabetes Care. 2025;48(00):1-9. doi:10.2337/dc24-2841 8. DeFronzo RA, Auchus RJ, Bancos I, et al. BMJ Open. 2024;14(7):e081121. doi:10.1136/bmjopen-2023-081121